![]() Men with poor semen quality;
Men with poor semen quality;
![]() Women with blocked or damaged fallopian tubes;
Women with blocked or damaged fallopian tubes;
![]() Couple with unexplained infertility, especially treatment with other methods has failed;
Couple with unexplained infertility, especially treatment with other methods has failed;
![]() Women with severe endometriosis;
Women with severe endometriosis;
![]() Women in their advanced reproductive age or low ovarian reserve, as time to conception is critical;
Women in their advanced reproductive age or low ovarian reserve, as time to conception is critical;
![]() Couples with an inherited genetic disease that they wish to avoid passing on to their child, and in this case, IVF is combined with preimplantation genetic testing (PGT) to select embryos without the disease for transfer.
Couples with an inherited genetic disease that they wish to avoid passing on to their child, and in this case, IVF is combined with preimplantation genetic testing (PGT) to select embryos without the disease for transfer.
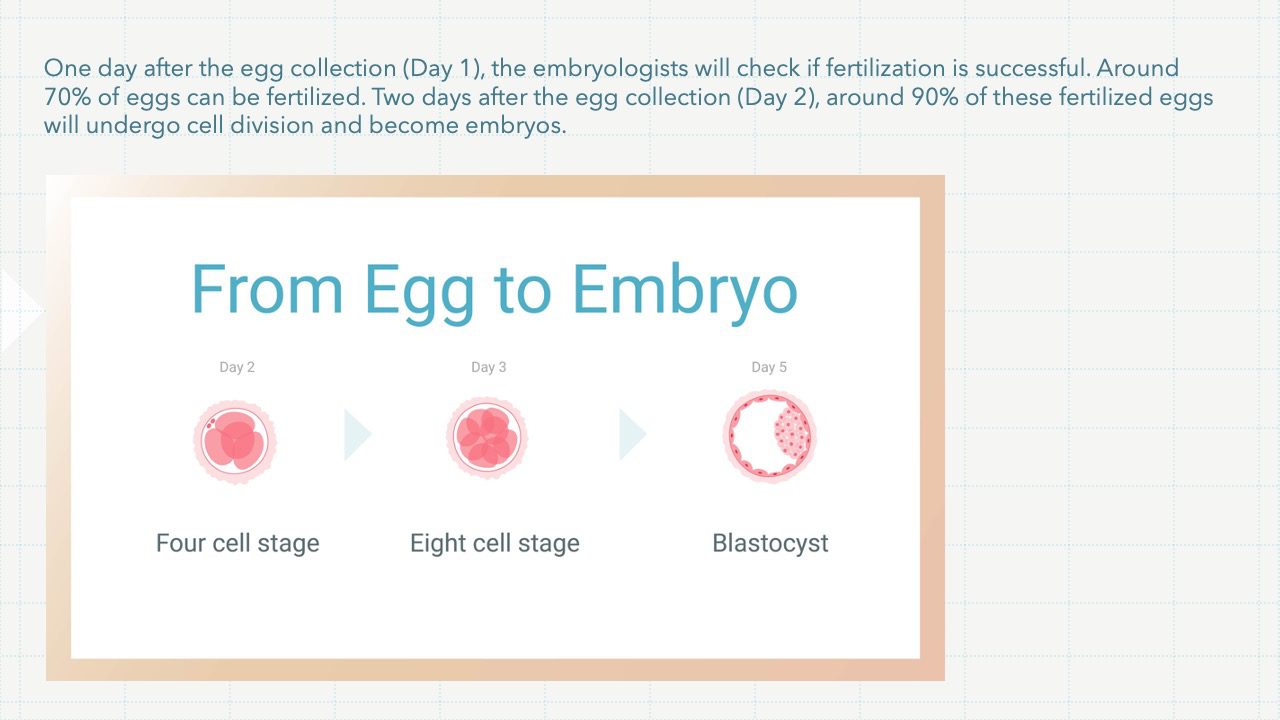
While the embryos are growing in the laboratory, you will need progesterone, and may be estrogen as well, to prepare the lining of the womb for embryo transfer. These are usually taken as pessaries which you can insert into the vagina yourself. The embryos will be ready to be returned to your womb 2 to 5 days after the egg collection (Day 2, Day 3 or Day 5). A small tube (catheter) is inserted through the cervix (the neck of the womb) and the embryo(s) is/are put into the womb cavity. Anaesthesia or analgesia is usually not required for this procedure. You can return to work on the same day or the next day. Your doctor may arrange a blood test a few days later to check your hormone levels to help decide if you need extra medications. You will be given a date to do a blood test for pregnancy, usually around 2 weeks after the egg collection.
Because of the risk of having a multiple pregnancy, only 1 or 2 embryo(s) will be put back into the womb. Under special situations, a maximum of 3 embryos can be replaced. Any remaining embryos that are of good quality will be frozen for use in the future, in case treatment does not work or to try for a sibling. They can be stored for up to a maximum of 10 years. Women in certain circumstances can store their embryos for up to 10 years or when they are 55 years old, whichever is later.
In a normal IVF cycle, the embryos can be returned to your womb a few days after the egg collection in the same cycle and any remaining suitable embryos are frozen. Your doctor may advise freezing all embryos for later transfer in another cycle if you have the following condition(s):
![]() Ovarian hyperstimulation syndrome (OHSS)
Ovarian hyperstimulation syndrome (OHSS)
![]() Your body’s hormonal response to stimulation drugs is affecting the lining of the womb, making it less receptive to embryo(s)
Your body’s hormonal response to stimulation drugs is affecting the lining of the womb, making it less receptive to embryo(s)
![]() You may have other medical condition that requires treatment before transferring the embryo(s) back to the womb
You may have other medical condition that requires treatment before transferring the embryo(s) back to the womb
![]() We work in collaboration with Hong Kong Assisted Reproduction Centre to provide IVF and related treatments.
We work in collaboration with Hong Kong Assisted Reproduction Centre to provide IVF and related treatments.
![]() Your FAQs answered :
Your FAQs answered :![]() Who should be considering IVF?
Who should be considering IVF?
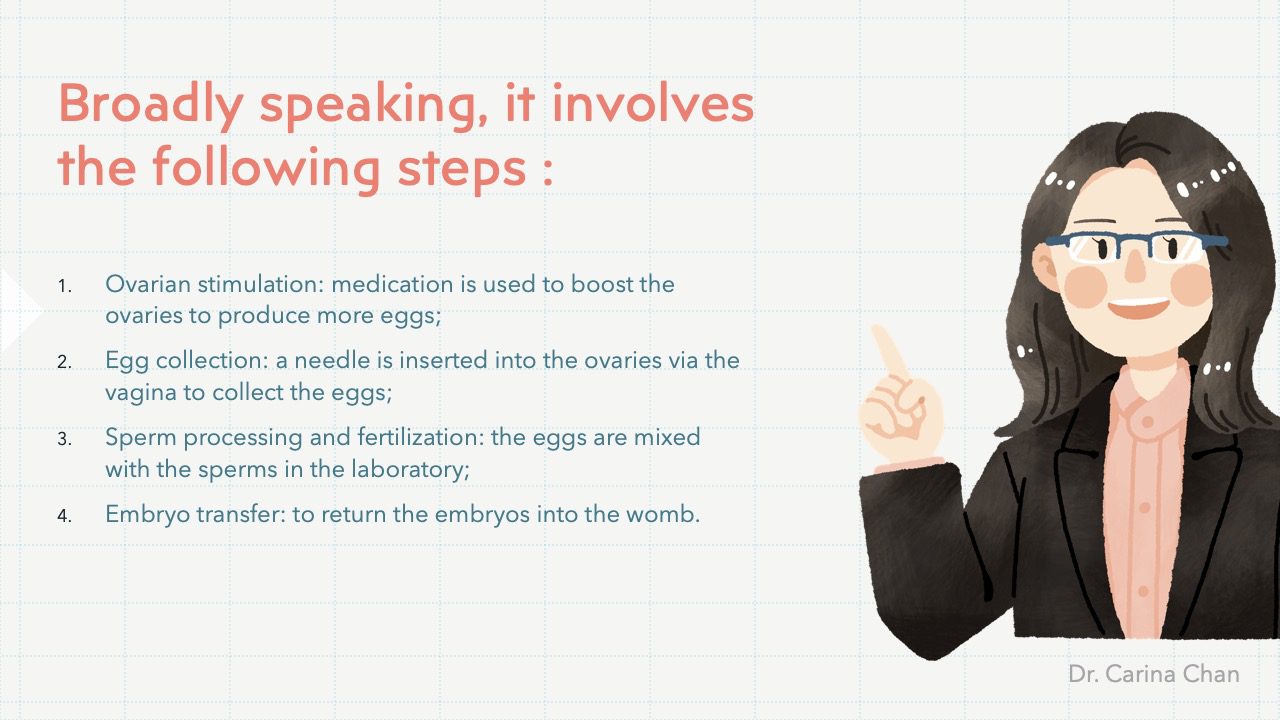
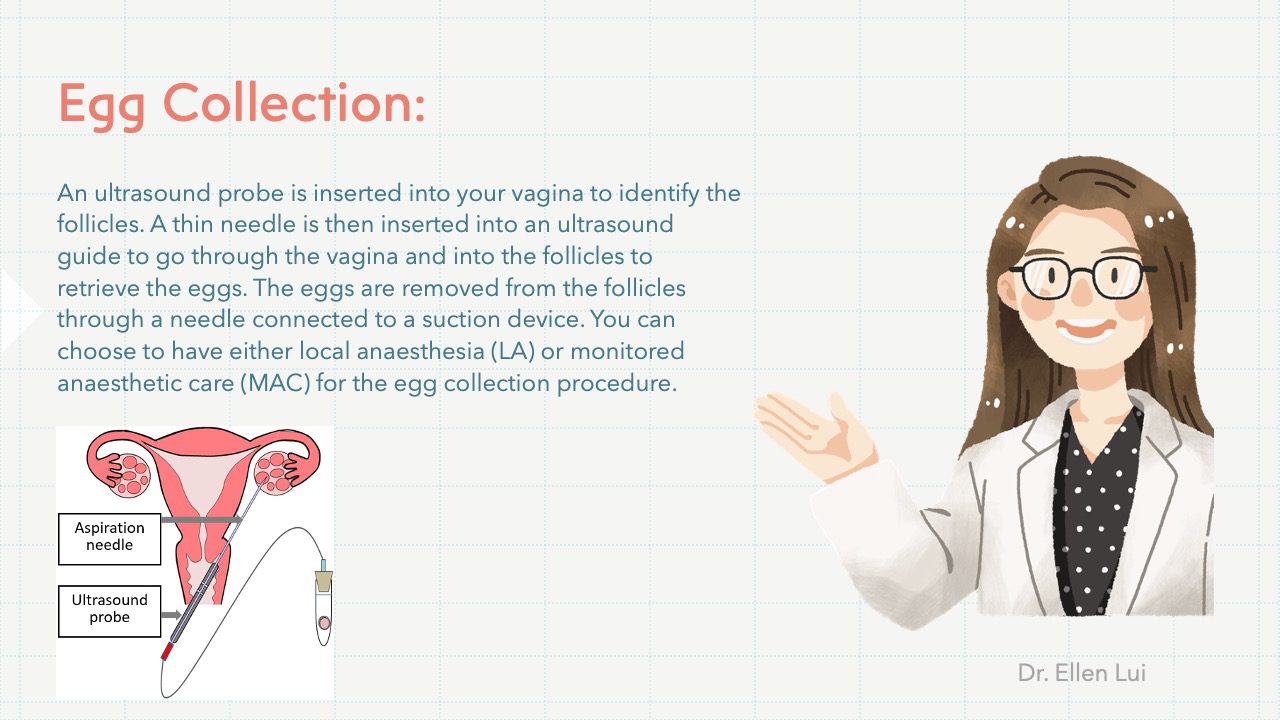
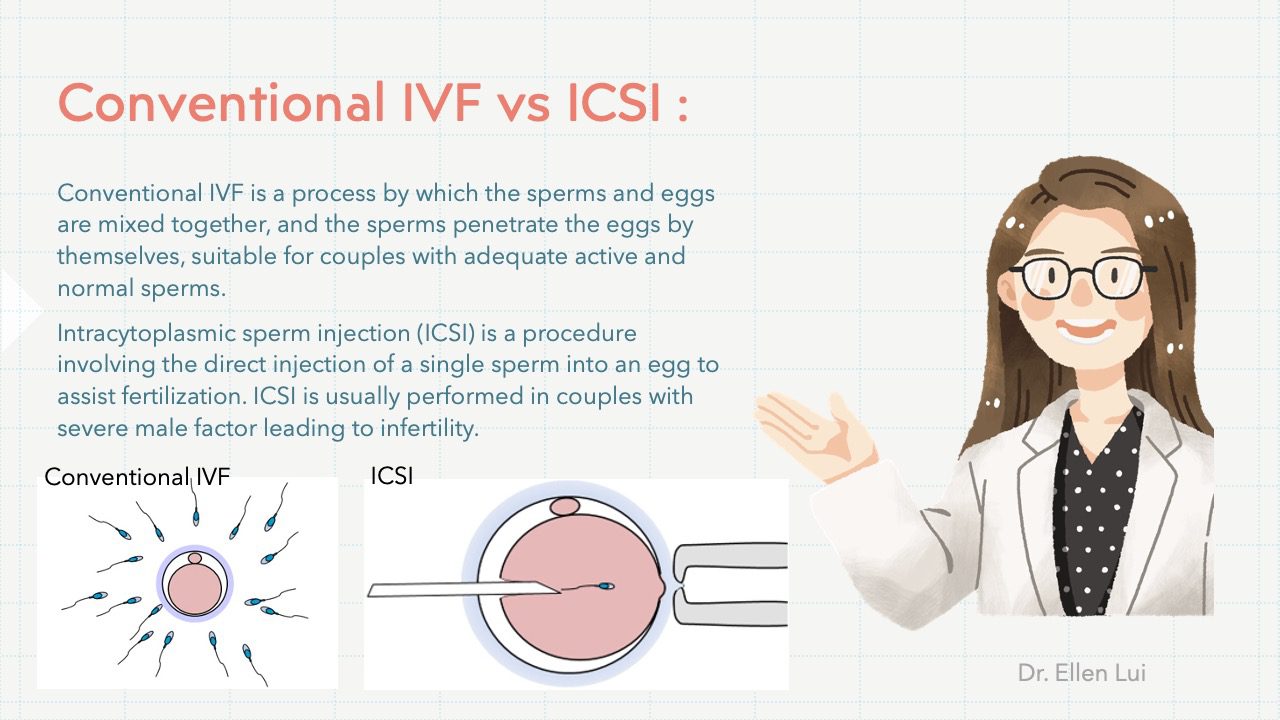
![]() What procedures are involved in IVF?
What procedures are involved in IVF?
![]() How many eggs will be generally collected?
How many eggs will be generally collected?
![]() How many embryos can be successfully implanted back to the wife?
How many embryos can be successfully implanted back to the wife?
![]() Is it good or bad to have twin pregnancy?
Is it good or bad to have twin pregnancy?
![]() What will happen to the surplus embryos?
What will happen to the surplus embryos?
![]() What should couples expect about the success rate?
What should couples expect about the success rate?
![]() How many times can couple try IVF?
How many times can couple try IVF?



{kind=link}